A 17 year old male was brought by his father with a history
of a painless, progressively increasing mass in the right eye since three months.
The patient was a known case of mild mental retardation. The patient was
receiving treatment for gingivitis in the form of tablet metronidazole from
dental department. The patient’s prenatal, perinatal, postnatal and family
histories were all unremarkable. There was no history of any other systemic
disease, trauma, seizures, ocular infection and surgery. His
visual acquity was 6/24 in both the eyes without any improvement on pinhole;
pupillary reactions, ocular movements, fundus and intraocular pressure were
normal bilaterally. Examination
of her right eye revealed a reddish, pedunculated, smooth, mobile mass with its surface revealing
multiple blood vessels. It was located in the bulbar conjunctiva near the
limbus at 8 o’clock position and was of 9mm x 8mm size (Figure 1). The slit
lamp examination of the left eye was normal. Routine blood and urine
examinations were normal. An excision biopsy of the mass under local
anaesthesia was planned. A preoperative general physical and systemic
examination was carried out by the medical specialist and a go ahead was given
for surgery. Excision biopsy of the mass was done (Figure 2) and the patient
was started on topical antibiotic-steroid eye drops. The patient reported back
to us after two weeks postoperatively along with the histopathological report
which revealed the conjunctival mass to be capillary hemangioma (Figure 3). The
patient was added timolol drops to decrease the incidence of recurrence of the
lesion.

Figure 1: Patients
Photograph Showing the Lesion.

Figure 2: Patients Photograph-First Postoperative Day.
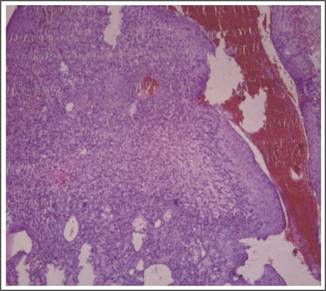
Figure 3: Histopathological Report.
DISCUSSION
Conjunctival vascular tumours are not common and a few examples of
the lesions commonly found in this group are pyogenic granuloma, lymphangioma,
and capillary hemangioma1. A haemangioma is a developmental malformation of
blood vessels and is an example of a hamartoma. It may be capillary, venous or
arterial. Its incidence is reported as 1-2% of all benign growths of the
conjunctiva2.
Conjuctival hemangiomas are
rare tumors3 which are
present at birth as reddish elevated lesions increasing in size over the next
few months and then spontaneously involuting by 4–5 years of age4.
These tumors can be asymptomatic or may cause visual impairment if large sized.
Capillary hemangiomas show a greater preponderence in females (especially with
a history of chorionic-villus sampling during pregnancy) and premature or
low-birth-weight infants. They have an association with cardiorespiratory and
hematologic disorders5.
Histopathological examination shows
proliferative vessels lined by endothelial cells without nuclear atypism. They
generally locate to the superior orbit and lids. Acquired capillary hemangioma
of the periocular region is very rare. The main differential diagnoses are
pyogenic granuloma, angiosarcoma, and acquired tufted angioma of the eyelids6.
The treatment modalities currently available include intralesional and
systemic steroids, bleomycin, interferon-α, topical timolol maleate, oral
propranolol, laser treatment and surgical excision7. Caution should
be taken in using beta blockers in patients of hemangioma with
cardiorespiratory disorders as worsening of respiratory and cardiac symptoms
can occur8.
Authors
Affiliation
Dr. Anubhav Chauhan
M.S Ophthalmology), Senior Resident, Dept. of Ophthalmology
Dr Yashwant Singh Parmar Govt. Medical College, Nahan, District
Sirmour, Himachal Pradesh, India.
Dr. Lalit Gupta
M.S Ophthalmology),Assistant Professor, Dept. of Ophthalmology
Dr Yashwant Singh Parmar Govt. Medical College, Nahan, District Sirmour, Himachal Pradesh, India.
Dr. Shveta Chauhan
Bachelor of Dental Surgery),Pine Castle, Near Mist Chamber, Khalini,
Shimla 171002, Himachal Pradesh, India
Role
of Authors
Dr. Anubhav Chauhan
Concept, Study design, Data acquisition and manuscript
writing.
Dr. Lalit Gupta
Drafting, Literature research and manuscript preparation
Dr. Shveta Chauhan
Manuscript editing, data analysis, and patient photographs
REFERENCES
1. Lubahn
JG, Lee RK, Karp CL. Resolution of Conjunctival Sessile Hemangioma with
Topical Timolol. Cornea 2014; 33 (1): 99–100.
2. Rao
MR, Patankar V L, Reddy V. Cavernous haemangioma of conjunctiva (a case
report). Indian J Ophthalmol. 1989; 37: 37-8.
3. Loya
N, Kremer I, Goldenfeld M, Swetliza E. Solitary Conjunctival Hemangioma
Presenting as a Chocolate Cyst. Arch Ophthalmol. 1988; 106 (10): 1457.
4. Honavar
SG, Manjandavida FP. Tumors of the ocular
surface:
A review. Indian J Ophthalmol. 2015; 63: 187-203.
5. Bang
GM, Setabutr P. Periocular Capillary Hemangiomas: Indications and Options
for Treatment. Middle East Afr J Ophthalmol. 2010 ; 17 (2): 121–128.
6. Kıvanç
SA, Olcaysu OO, Gelincik I. Acquired capillary hemangioma of the eyelid in
a 49-year-old woman from Turkey. Indian J Ophthalmol. 2014; 62 (9): 969–970.
7. Ohnishi
K, Tagami M, Morii E, Azumi A. Topical Treatment for Orbital Capillary
Hemangioma in an Adult Using a β-Blocker Solution. Case Rep Ophthalmol.
2014; 5: 60-65.
8. Ambika
H, Sujatha C, Kumar YH. Topical Timolol: A Safer Alternative for
Complicated and UnComplicated Infantile Hemangiomas. Indian J Dermatol. 2013;
58 (4): 330.